Insights
Sciatica or Back Pain? How to Tell the Difference (And Why It Changes Your Treatment)

Most people use the words interchangeably. Their back hurts, they call it sciatica. Or a provider tells them they have sciatica, and they assume it just means their back is giving them trouble. For the purposes of describing discomfort, that imprecision is forgivable.
For the purposes of treatment, it can mean the difference between getting better and spinning in circles for months.
Sciatica and lower back pain often occur together, often share overlapping symptoms, and often get treated identically by providers who did not take the time to distinguish them. But they have different sources, different mechanisms, and different treatment priorities. Getting that distinction right at the start is one of the most important things a chiropractor in Tallahassee can do for a patient walking in with pain that runs from the low back down through the leg.
What Lower Back Pain Actually Is
Lower back pain, in the broadest clinical sense, refers to pain that originates in the structures of the lumbar spine and surrounding musculature — without necessarily involving the sciatic nerve. Sources include:
• Facet joint dysfunction: Irritation or degeneration of the small joints connecting each vertebra, producing localized stiffness and aching, often worse with extension or prolonged standing.
• Muscular strain and trigger points: Acute or chronic overloading of the paraspinal muscles, producing tightness, tenderness, and restricted range of motion — the most common presentation after a sudden awkward lift or prolonged poor posture.
• Sacroiliac (SI) joint dysfunction: Irritation of the joint connecting the sacrum to the pelvis, producing pain at or just below the beltline on one or both sides, sometimes mistaken for a disc problem or hip issue.
• Disc degeneration without nerve involvement: Wear-related changes to the discs between vertebrae that reduce disc height and alter spinal mechanics — painful, but not necessarily producing nerve symptoms unless a nerve root is compressed.
Pure lower back pain, regardless of its source, tends to stay in the back. It may radiate slightly into the buttocks or upper thigh, but it does not typically travel below the knee, and it does not produce the characteristic neurological sensations that define sciatica.
What Sciatica Actually Is
Sciatica is not a diagnosis in the same way that lower back pain is. Sciatica is a symptom pattern — specifically, pain, tingling, numbness, or weakness that travels along the path of the sciatic nerve, which runs from the lower lumbar spine through the buttocks, down the back of each leg, and into the foot.
According to the National Institute of Neurological Disorders and Stroke (NINDS), sciatica affects an estimated 40 percent of adults at some point in their lifetime, most commonly between the ages of 30 and 50. The underlying cause is almost always compression or irritation of one or more nerve roots that form the sciatic nerve — most frequently from a herniated lumbar disc, but also from bone spurs, spinal stenosis, or piriformis muscle compression.
What distinguishes sciatica from general back pain is the nerve involvement. Sciatica produces symptoms in a specific pattern that follows the path of the affected nerve root — a pattern clinicians call a dermatomal distribution. Pain, burning, or numbness in a stripe along the outer calf and into the top of the foot suggests L5 nerve root involvement. Symptoms running down the back of the calf and into the heel suggest S1 involvement. These distinctions matter because they point to specific levels of the spine where compression is likely occurring.
Side-by-Side: How They Feel Differently
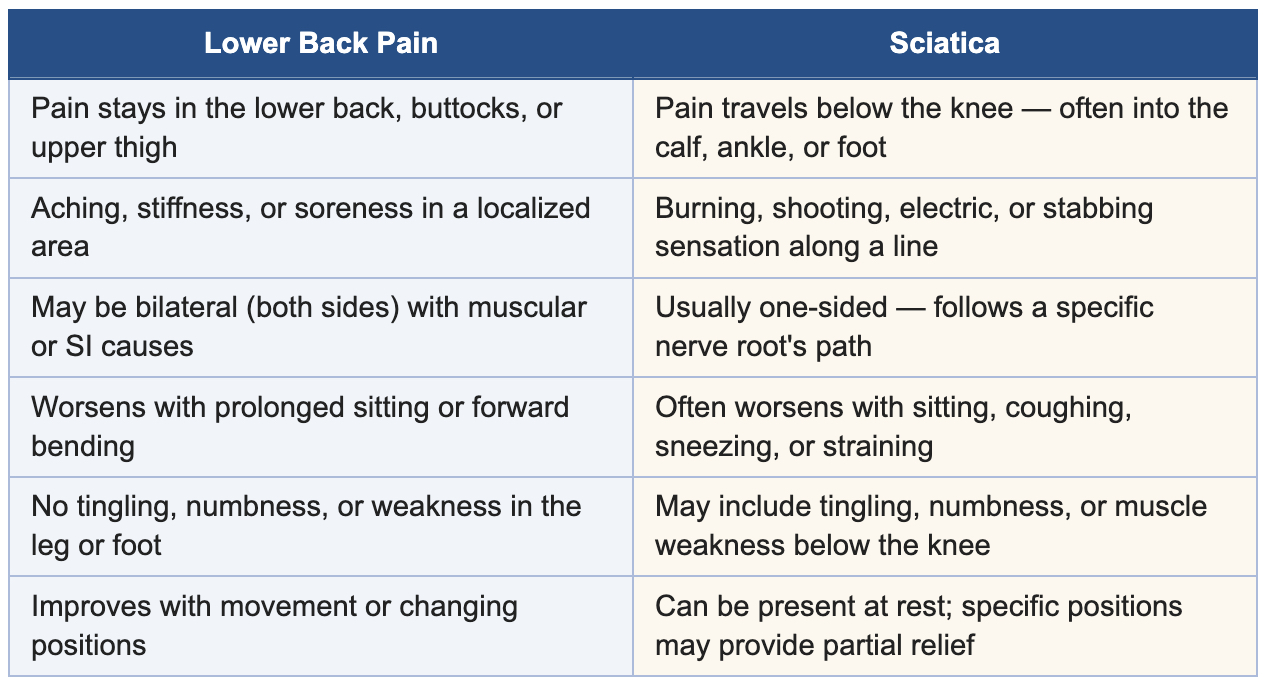
One important caveat: sciatica almost always includes a component of lower back pain or buttock pain alongside the leg symptoms. The presence of lower back pain does not rule sciatica out. What rules it in is the nerve symptom pattern that extends below the knee.
Why the Distinction Changes Treatment
Treating sciatica with the same protocol used for a muscular lower back strain — rest, heat, anti-inflammatories, and general massage — rarely produces lasting relief. Here is why.
Sciatica Requires Addressing the Nerve Root, Not Just the Muscle
When sciatica originates from a herniated lumbar disc, the goal of care is to reduce the pressure on the affected nerve root — through spinal manipulation targeted at restoring disc mechanics, specific traction or decompression techniques, and rehabilitation exercises that reduce nuclear pressure on the disc wall. General massage or heat applied to the lumbar muscles may feel temporarily soothing, but it does not decompress the nerve root causing the radiating pain.
A systematic review published in the Journal of Orthopaedic and Sports Physical Therapy found that direction-specific exercises — particularly extension-based movements in patients with posterolateral disc herniation — produced significantly greater pain reduction and faster neurological recovery than non-specific general exercise. Getting the direction of rehabilitation right requires knowing which nerve root is involved and which disc level is responsible.
The Cause of Sciatica Determines the Approach
Sciatica from a herniated disc, sciatica from piriformis syndrome, and sciatica from lumbar spinal stenosis all share the same symptom pattern but require meaningfully different treatment priorities:
• Disc herniation: Responds well to spinal manipulation, flexion-distraction techniques, extension-biased rehabilitation, and nerve mobilization. Avoiding prolonged sitting and forward flexion is critical early in care.
• Piriformis syndrome: The sciatic nerve is compressed by the piriformis muscle deep in the buttock — not by the spine at all. Treatment focuses on soft-tissue release, piriformis stretching, hip external rotator strengthening, and addressing the hip mechanics driving the muscle overload.
• Lumbar spinal stenosis: Narrowing of the spinal canal that compresses nerve roots, often in older adults, producing symptoms that worsen with walking and improve with sitting or forward flexion. Flexion-biased rehabilitation, aquatic therapy, and in some cases surgical consultation are appropriate depending on severity.
Applying the wrong protocol to any of these three causes — or applying a generic lower back pain protocol to any of them — explains why so many patients cycle through treatment without lasting relief.
Chiropractic Evaluation Identifies Which Type You Have
At University Physical Medicine in Tallahassee, every patient presenting with leg pain, buttock pain, or lower back pain that radiates receives a structured neurological and orthopedic examination designed to answer the right questions before any treatment begins. Straight leg raise testing, slump testing, dermatomal sensory mapping, reflex assessment, and provocative disc and facet testing are all part of differentiating the source.
For patients with confirmed or suspected disc herniation, chiropractic care for sciatica in Tallahassee is built around reducing nuclear disc pressure through specific manipulation techniques, targeted rehabilitation, and postural re-education. For patients whose imaging reveals significant stenosis or whose neurological deficits are progressing, appropriate referral for surgical consultation is part of the care decision — an honest integrated team will never over-treat beyond what conservative care can reasonably achieve.
The Role of Disc Injury in Both Conditions
A herniated or bulging disc is the single most common link between lower back pain and sciatica. When a disc herniates posterolaterally, it can simultaneously produce local back pain from disc and facet irritation and nerve root symptoms from direct compression of an adjacent nerve — meaning a patient may have both conditions originating from a single injury.
According to the American Academy of Orthopaedic Surgeons (AAOS), most patients with lumbar disc herniation and sciatica improve significantly with conservative care within six to twelve weeks. Surgery is rarely required and is typically reserved for patients with progressive neurological deficits, bowel or bladder involvement, or failure to improve after an adequate trial of conservative management.
For patients navigating a disc injury in Tallahassee, the most important early steps are accurate diagnosis of which disc is involved, confirmation of the direction of herniation, and a care plan built around reducing neural tension and restoring controlled movement — not rest alone.
When Adjunct Therapies Add Value
For patients with sciatica or recurrent lower back pain, chiropractic adjustments and targeted rehabilitation are the core of the care plan. Certain adjunct therapies extend and support that core effectively when selected for the right patient and the right presentation:
• Shockwave therapy: For patients with associated piriformis syndrome or deep gluteal muscle involvement, shockwave therapy can help reduce muscular tension and improve tissue healing in the soft-tissue components contributing to sciatic nerve compression.
• Class IV laser therapy: Photobiomodulation has shown supportive evidence for reducing nerve-related pain and inflammatory markers in soft tissue adjacent to irritated nerve roots — useful as part of a broader protocol rather than as a standalone intervention.
• Intersegmental traction and therapeutic ultrasound: Both help maintain disc hydration, improve joint mobility, and reduce paraspinal muscle tension during the active phase of care, supporting the spinal manipulation component of treatment.
Red Flags: When Sciatica or Back Pain Needs Emergency Evaluation
• Sudden loss of bladder or bowel control — may indicate cauda equina syndrome, a surgical emergency requiring immediate ER care
• Rapid or progressive weakness in one or both legs that is worsening day over day
• Numbness or tingling in the saddle area (groin, inner thighs, perineum) following trauma
• Back pain with fever, chills, or unexplained weight loss — may indicate infection or systemic pathology
• Severe back pain immediately following significant trauma such as a fall, accident, or sports collision
What Patients in Tallahassee Are Missing
Most patients who come into University Physical Medicine with unresolved sciatica or recurrent back pain share one thing in common: they were treated for a symptom instead of a diagnosis. Pain was addressed without a clinical examination that mapped which nerve root was involved, which structure was compressing it, or which movement patterns were sustaining the problem.
According to Florida Health, Leon County, musculoskeletal pain conditions are among the leading drivers of reduced functional capacity and healthcare utilization across the Tallahassee area. Access to precise, diagnosis-first care — rather than generic pain management — represents one of the most meaningful gaps in how most patients navigate these conditions locally.
Getting the right answer about whether you have sciatica, pure lower back pain, or both — and which specific structure is driving it — is not a minor clinical detail. It is the difference between a care plan that works and one that manages symptoms until the next flare.
Frequently Asked Questions
Q: Can sciatica go away on its own without treatment?
A: Mild sciatica from a small disc herniation sometimes resolves over six to twelve weeks as the disc material reabsorbs and inflammation subsides. However, without addressing the mechanical dysfunction and movement patterns that contributed to the herniation, recurrence is common. Patients with moderate to severe symptoms, neurological findings, or pain lasting beyond four to six weeks benefit from active clinical intervention rather than watchful waiting alone.
Q: How does a chiropractor diagnose sciatica versus back pain?
A: A thorough clinical examination includes orthopedic provocation tests like the straight leg raise and slump test, dermatomal sensory mapping to identify the specific nerve root involved, deep tendon reflex testing, and muscle strength grading. Range of motion, postural assessment, and a detailed symptom history — including exactly where the pain travels and what positions aggravate or relieve it — complete the clinical picture. Imaging is ordered when the examination suggests it will change the treatment plan.
Q: My pain only goes to my buttock and upper thigh — is that sciatica?
A: Not necessarily. Referred pain from the sacroiliac joint, the lower facet joints, or the gluteal musculature can mimic early sciatica and produce symptoms in the buttock and upper thigh without true nerve root involvement. Distinguishing between referred pain and true radiculopathy requires a structured clinical examination — the treatment approach for each is meaningfully different.
Q: Will I need an MRI to find out if I have sciatica?
A: An MRI is the most informative imaging study for diagnosing disc herniation and nerve root compression. However, imaging is not always required before beginning conservative care. If your clinical examination clearly points to the likely level and cause, treatment can begin while imaging is arranged. An MRI becomes more important when symptoms are severe, progressive, or not responding to initial conservative care — or when the clinical picture is ambiguous.
Q: How long does sciatica treatment take at an integrated chiropractic practice?
A: Most patients with acute sciatica from disc herniation notice meaningful improvement within four to eight weeks of consistent care. Chronic cases with significant disc degeneration or spinal stenosis typically require a longer care timeline with ongoing maintenance. The honest answer depends on the specific cause, how long the condition has been present, and how fully the patient engages with the rehabilitation component alongside adjustments.
Get a Diagnosis — Not Just a Label
Whether your pain stays in your back, runs down your leg, or does both, the first step toward lasting relief is knowing what is actually causing it. University Physical Medicine's integrated clinical team in Tallahassee evaluates sciatica and lower back pain with the diagnostic precision that most patients never receive at their first point of contact.
Dr. Belletto and the UPM team see new patients at 1224 Ocala Rd — one mile from FSU and TCC — with same-day appointments typically available.
Schedule your evaluation today or call (850) 576-2129 to speak with our team directly.
University Physical Medicine | 1224 Ocala Rd, Tallahassee, FL 32304
Mon / Wed / Thu: 8:30 AM – 5:30 PM | Tue / Fri: 8:30 AM – 12:30 PM
Medical Disclaimer: This article is for general informational purposes only and does not constitute medical advice, diagnosis, or treatment. Sciatica and back pain have multiple potential causes, and an accurate diagnosis requires a clinical evaluation by a licensed healthcare provider. If you are experiencing progressive leg weakness, loss of bladder or bowel control, or numbness in the saddle area, seek emergency care immediately.Q:Q:Q